
The role of anthracyclines in small cell lung cancer
Key words: Small cell lung cancer; anthracyclines; amrubicin
Introduction
Prognosis at relapse is poor and response to second-line chemotherapy is correlated with response to first-line therapy and the interval between first-line chemotherapy and disease progression (1). Patients who relapse less than three months after fist-line therapy are commonly called “refractory” and have response rates than are lower than those of patients who relapse more than three months after therapy, who are usually called “sensitive” (2). There is no standard second-line therapy for SCLC.
In 2009, a meta-analysis about chemotherapy versus best supportive care (BSC) for extensive small cell lung cancer was published by the Cochrane Lung Cancer Group (3). The review included phase III randomised trials both first and second line. Two studies in first line and two studies in second line were analyzed. In the first line (4,5), both studies compared ifosfamide +/- CCNU vs. BSC, showing a benefit in overall survival between chemotherapy vs. BSC (P=0.01) with no differences adding CCNU. In the second line, chemotherapy also show benefit in overall survival [methotrexate-doxorubicin vs. BSC P<0.001 (6); topotecan vs. BSC P=0.01 (7)].
Doxorubicin-based chemotherapy as second line therapy for SCLC
Doxorubicin-based chemotherapy was widely used in Europe as a reference regimen for first line therapy in SCLC (8), and so for the European Organisation for Research and Treatment of Cancer (EORTC) Lung Group. Median survival of 9 to 11 months with 1 year survival of 30-40% were reported in patients with good PS (9). However, cisplatin and etoposide were widely used in North America, with similar survival rates to those reported for doxorubicin-based chemotherapy (10).
The first trial comparing cisplatin-based chemotherapy and doxorubicin-based chemotherapy was published in 2002 by Sundstrom et al. (11). A total of 436 patients were randomized to chemotherapy with cisplatin-etoposide (EP) or ciclophosphamide, epirubicin and vincristine (CEV). Patients were stratified according to limited disease or extensive disease. The two and five year survival rates in the EP arm were significantly higher compared with those in the CEV arm (14% and 5% vs. 6% and 2%, P=0.0004).
A few years later, Baka et al. published a phase III trial comparing six cycles of doxorubicin, cyclophosphamide and etoposide (ACE) vs. six cycles of EP (12). A total of 280 patients were included, 60% limited stage and 40% extensive disease. No differences were observed between the two groups in one year survival rates (34% vs. 38%, P=0.51) and in two year survival (12% vs. 12%). However, the ACE group was associated with a higher risk of neutropenic sepsis (90% vs. 57%, P<0.005).
There is also a meta-analysis of the randomized trials of a cisplatin-containing regimen versus a regimen without platinum (13). Ten trials randomized patients to receive a cisplatin-etoposide regimen versus a regimen without any of these two drugs. Patients treated with a cisplatin-containing regimen benefited from a significant reduction of risk of death at 6 months (OR 0.87, P=0.03) and 1 year (OR 0.80, P=0.002).
After that, cisplatin-based chemotherapy was stablished as the standard of first line therapy, both limited stage and in extensive stage, and so, doxorubicin-based chemotherapy took a second place in the treatment of SCLC.
In 2007, a systematic review was published about chemotherapy for relapsed SCLC; it was developed by Cancer Care Ontario’s Program in Evidence-base Care (14). Six randomized trials were included for review. The first phase III trial compared oral topotecan vs. best supportive care and it demonstrated a significant survival benefit (HR 0.64; P=0.01) (15). It was the first trial to demonstrate a significant improvement in overall and median survival and quality of life in patients with relapsed SCLC, favoring treatment with topotecan vs. BSC. Three randomized trials have compared different chemotherapy regimens with no differences in median survival between them (cisplatin-etoposide vs. carboplatin-cisplatin-etoposide; cyclophosphamide-doxorubicin-vincristine vs. topotecan; cisplatin-etoposide vs. nitrosourea-thiotepa-vincristine-cyclophosphamide) (16-18). One phase II and one phase III trial compared the oral and intravenous administration of topotecan, reporting similar response and median survival rates; nevertheless, neutropenia was higher in the intravenous arm.
There is limited evidence for determining which patients are the best to benefit from second-line chemotherapy. In general, a poor PS (≥2) and relapse within six weeks of completing first-line chemotherapy are recognized as poor prognostic factors, and they are related to lower response rates and shorter survival in SCLC (9).
Doxorubicin combinations vs. topotecan
Topotecan as a single agent has been studied in several phase II trials as second-line therapy for SCLC, reporting a median survival around 25 weeks (19-21). Also a meta-analysis of these phase II trials was made, showing a 18% response rate and median survival of 30 weeks (22). Based on these results, a phase III randomized trial was performed with cyclophosphamide, doxorubicin and vincristine in the control arm (23).
211 patients were treated in the study, all of them had relapsed at least 60 days after completion of first-line therapy. No difference were found in response rate (24% vs. 18%, P=0.28), median times to progression (13 vs. 12 weeks, P=0.05) and median survival (25 vs. 24 weeks, P=0.79). Talking about toxicity, grade 4 neutropenia was higher in the CAV group (37% vs. 51%, P<0.001), but grade 4 thrombocytopenia and grade 4 anemia was higher in the topotecan group (9.8% and 17% vs. 1.4% and 7.2%, P=0.001). Non-hematologic toxicities were similar for both regimens. It was the only study to report improvement, (but not statistically significant) in symptom management with topotecan compared with CAV. However, the scoring system for this measure was not validated.
Amrubicin: next-generation anthracycline for the management of SCLC
Mechanism of action and preclinical studies
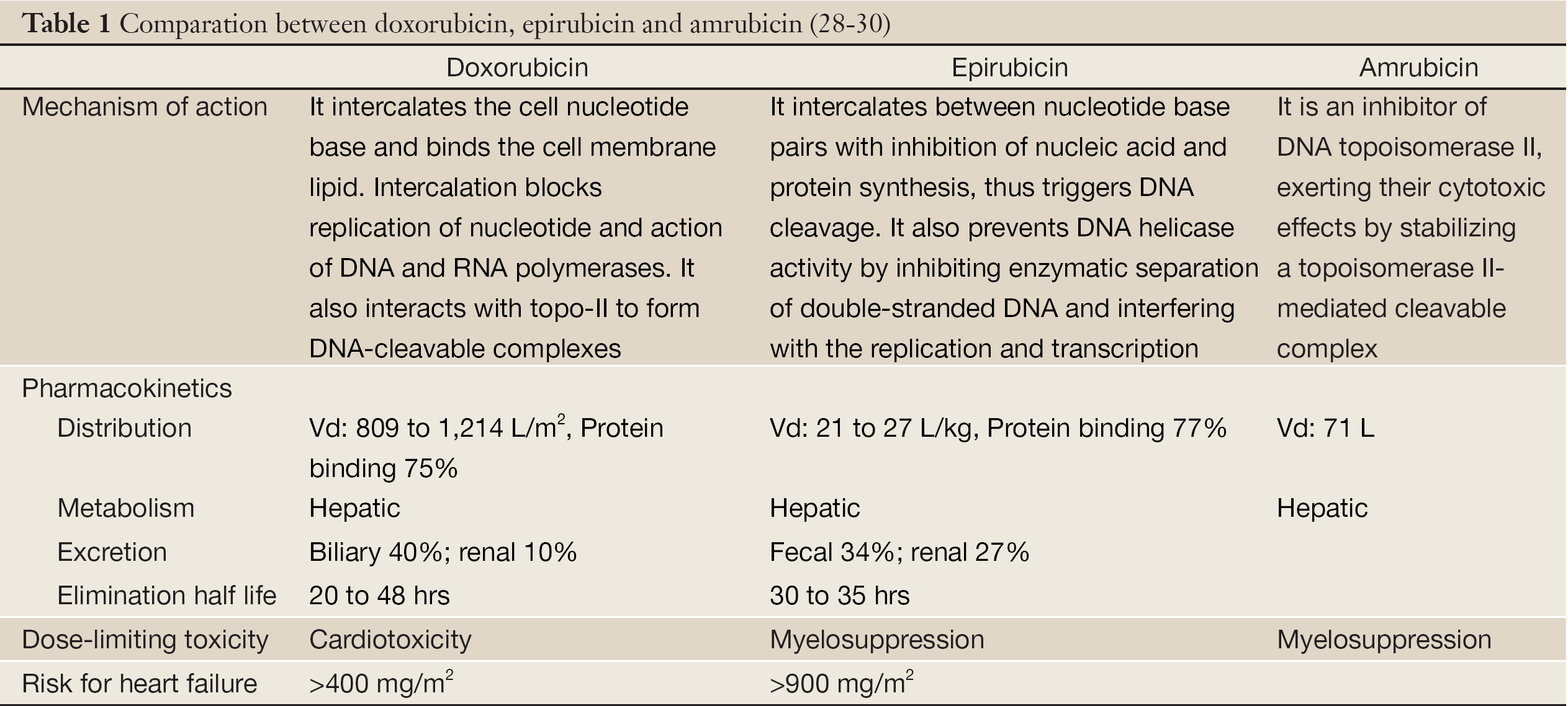
Amrubicin is a totally synthetic anthracycline. It is converted to amrubicinol through the reduction of its C-13 ketone group to a hydroxyl group, which is up to 200 times more potent. Its mode of action is different from that of doxorubicin. It is an inhibitor of DNA topoisomerase II, exerting their cytotoxic effects by stabilizing a topoisomerase II-mediated cleavable complex.
In vitro experiments, amrubicin and its metabolite amrubicinol have been found to be active against a broad spectrum of human cell lines established from cancers of the lung, prostate, urinary bladder, colon, kidney, pancreas, and uterus (24).
Amrubicin has been shown to be more effective against 5 human xenografts, including lung cancer, compared with doxorubicin (25).
Noguchi et al. showed in 1998 that amrubicinol has more potent antitumor activity than amrubicin, in mice experiments (26). And the most interesting finding, the levels of amrubicinol in the tumors of these mice were higher than doxorubicin levels in doxorubicin-treated mice. However, in several non-tumor tissues, including the heart, the levels of amrubicin and amrubicinol were lower than those of doxorubicin. Also, a good correlation was found between the lever of amrubicinol in the tumor and the efficacy of amrubicin in vivo.
Cardiotoxicity is one of the dose-limiting toxicities of anthracyclines. Comparing with doxorubicin, amrubicin showed lower cardiotoxicity at equivalent dosages in rabbits (27). This seems to be due to the restricted distribution of the active metabolite in non-tumor tissues.
In Table 1, the principal differences between amrubicin and the more frequently anthracyclin used, are shown (31).
Amrubicin as a single agent
A phase I trial employed a single intermittent schedule of doses escalating from 10 to 130 mg/m2 in six steps. Leukopenia was the dose-limiting toxicity and the highest dose was the maximum tolerated dose. Digestive adverse-effects were milder than those induced by doxorubicin. The recommended dose for phase II trials was determined to be 100 mg/m2 given every three weeks (32). Next, Okamoto et al. (33) conducted a phase I study for refractory or relapsed lung cancer (NSCLC or SCLC) with fifteen patients, at doses of 30, 35 or 40 mg/m2 on three consecutive days every three weeks. The maximum tolerated dose and recommended dose were determined as 40 and 35 mg/m2, respectively. Grade 4 neutropenia was observed in 67%.
A phase II trial was conducted to look for the activity of amrubicin for the treatment of refractory or relapsed SCLC (34). 60 patients were enrolled between June 2003 and December 2004. The median number of treatment cycles was four. The overall response rates were 50% in the refractory group, and 52% in the sensitive group. The progression-free survival, overall survival and one year survival in the refractory group and the sensitive group were 2.6 and 4.2 months, 10.3 and 11.6 months, and 40% and 46%, respectively. The most frequent toxicity was myelosuppresion, which affected leukocytes primarily.
Two randomized phase II trials were performed in order to compare amrubicin vs. topotecan as second line treatment in patients with SCLC (35,36). The first of them was published in 2008 with 60 patients enrolled. ORR was 38% for the amrubicin arm and 13% for the topotecan arm in the sensitive relapse. Median PFS was 3.5 months for patients in the amrubicin arm and 2.2 months for patients in the topotecan arm. In the second one, 76 patients participated in the trial; once again, amrubicin resulted in a significantly higher ORR than topotecan (44% vs. 15%, P=0.021) and tolerability was similar with both agents. Neutropenia and thrombocytopenia grade 3 or worse was more frequent in the topotecan group.
Amrubicin-based chemotherapy
As several studies have suggested the efficacy of combination regimens for relapsed SCLC, and based in the results of the studies previously reported, a randomized phase II trial exploring the combination of amrubicin and topotecan (37).
59 patients participated in the study, 31 chemotherapy-naïve and 28 relapsed. Talking about second lines, in the relapsed group the median progression-free survival time and median survival time was 4.7 and 10.2 months, with a 27% of ORR. The main toxicity found was myelosuppresion with grades 3 or 4 neutropenia in 97% of the patients.
To our knowledge, there are three phase III clinical studies exploring amrubicin; one monotherapy trial with SCLC patients after failure of first-line chemotherapy, comparing amrubicin with topotecan; and two double combination regimen trials: a randomized, multicenter study comparing irinotecan with cisplatin versus amrubicin with cisplatin in patients with extensive-disease SCLC, and a study of amrubicin with cisplatin versus etoposide with cisplatin in extensive disease SCLC patients.
Current situation of amrubicin
On April 2008, orphan designation was granted by the European Medicines Agency for amrubicin (38). Previously it was been accepted in Japan as an option for treatment extensive disease SCLC. The orphan medicinal product designation is based on the seriousness of the condition, the existence of alternative methods of treatment and the rarity of the condition (affecting not more than 5 in 10,000 people in the EU; SCLC affects to less than 1.5 in 10,000 people in the EU) or insufficient returns on investment.
The orphan medicinal products are still under investigation, and they are considered for an orphan designation due to the potential activity; the orphan designation is not a marketing authorisation, a demonstration of quality, safety and efficacy is needed before.
Results from the phase III trials previously appointed are being expected for a possible approval.
Conclusions
Anthracyclines are active in SCLC, both as a single agent and also in combination. The combination CAV is as effective as topotecan in the second line therapy with different toxicity. The synthetic anthracyclin amrubicin shows good results in phase II trials compared with topotecan that should be confirmed in future phase III trials, with less cardiotoxicity than doxorubicin.
Acknowledgements
Disclosure: The authors declare no conflict of interest.
References
- Giaccone G, Donadio M, Bonardi G, et al. Teniposide in the treatment of small-cell lung cancer: the influence of prior chemotherapy. J Clin Oncol 1988;6:1264-70.
- Ardizzoni A, Hansen H, Dombernowsky P, et al. Topotecan, a new active drug in the second-line treatment of small-cell lung cancer: a phase II study in patients with refractory and sensitive disease. The European Organization for Research and Treatment of Cancer Early Clinical Studies Group and New Drug Development Office, and the Lung Cancer Cooperative Group. J Clin Oncol 1997;15:2090-6.
- Pelayo Alvarez M, Gallego Rubio O, Bonfill Cosp X, et al. Chemotherapy versus best supportive care for extensive small cell lung cancer. Cochrane Database Syst Rev 2009;(4):CD001990.
- Kokron O, Titscher R, Micksche M, et al. Clinical experiences with Holoxan in small cell carcinoma of the bronchus (author’s transl). Osterr Z Onkol 1977;4:103-6.
- Kokron O, Micksche M, Titscher R, et al. Ifosfamide versus ifosfamide + CCNU in the treatment of inoperable small cell carcinoma of the lung. A clinical study. Onkologie 1982;5:56-9.
- Spiro SG, Souhami RL, Geddes DM, et al. Duration of chemotherapy in small cell lung cancer: a Cancer Research Campaign trial. Br J Cancer 1989;59:578-83.
- O’Brien ME, Ciuleanu TE, Tsekov H, et al. Phase III trial comparing supportive care alone with supportive care with oral topotecan in patients with relapsed small-cell lung cancer. J Clin Oncol 2006;24:5441-7.
- Thatcher N, Girling DJ, Hopwood P, et al. Improving survival without reducing quality of life in small-cell lung cancer patients by increasing the dose-intensity of chemotherapy with granulocyte colony-stimulating factor support: results of a British Medical Research Council Multicenter Randomized Trial. Medical Research Council Lung Cancer Working Party. J Clin Oncol 2000;18:395-404.
- Giaccone G, Dalesio O, McVie GJ, et al. Maintenance chemotherapy in small-cell lung cancer: long-term results of a randomized trial. European Organization for Research and Treatment of Cancer Lung Cancer Cooperative Group. J Clin Oncol 1993;11:1230-40.
- Roth BJ, Johnson DH, Einhorn LH, et al. Randomized study of cyclophosphamide, doxorubicin, and vincristine versus etoposide and cisplatin versus alternation of these two regimens in extensive small-cell lung cancer: a phase III trial of the Southeastern Cancer Study Group. J Clin Oncol 1992;10:282-91.
- Sundstrøm S, Bremnes RM, Kaasa S, et al. Cisplatin and etoposide regimen is superior to cyclophosphamide, epirubicin, and vincristine regimen in small-cell lung cancer: results from a randomized phase III trial with 5 years’ follow-up. J Clin Oncol 2002;20:4665-72.
- Baka S, Califano R, Ferraldeschi R, et al. Phase III randomised trial of doxorubicin-based chemotherapy compared with platinum-based chemotherapy in small-cell lung cancer. Br J Cancer 2008;99:442-7.
- Pujol JL, Carestia L, Daurès JP. Is there a case for cisplatin in the treatment of small-cell lung cancer? A meta-analysis of randomized trials of a cisplatin-containing regimen versus a regimen without this alkylating agent. Br J Cancer 2000;83:8-15.
- Cheng S, Evans WK, Stys-Norman D, et al. Chemotherapy for relapsed small cell lung cancer: a systematic review and practice guideline. J Thorac Oncol 2007;2:348-54.
- O’Brien ME, Ciuleanu TE, Tsekov H, et al. Phase III trial comparing supportive care alone with supportive care with oral topotecan in patients with relapsed small-cell lung cancer. J Clin Oncol 2006;24:5441-7.
- Sculier JP, Lafitte JJ, Lecomte J, et al. A phase II randomised trial comparing the cisplatin-etoposide combination chemotherapy with or without carboplatin as second-line therapy for small-cell lung cancer. Ann Oncol 2002;13:1454-9.
- von Pawel J, Schiller JH, Shepherd FA, et al. Topotecan versus cyclophosphamide, doxorubicin, and vincristine for the treatment of recurrent small-cell lung cancer. J Clin Oncol 1999;17:658-67.
- O’Bryan RM, Crowley JJ, Kim PN, et al. Comparison of etoposide and cisplatin with bis-chloro-ethylnitrosourea, thiotepa, vincristine, and cyclophosphamide for salvage treatment in small cell lung cancer. A Southwest Oncology Group Study. Cancer 1990;65:856-60.
- Ardizzoni A, Hansen H, Dombernowsky P, et al. Topotecan, a new active drug in the second-line treatment of small-cell lung cancer: a phase II study in patients with refractory and sensitive disease. The European Organization for Research and Treatment of Cancer Early Clinical Studies Group and New Drug Development Office, and the Lung Cancer Cooperative Group. J Clin Oncol 1997;15:2090-6.
- Depierre A, von Pawel J, Hans K et al. Evaluation of topotecan (HycamtinTM) in relapsed small cell lung cancer (SCLC): a multicentre phase II study. Lung Cancer 1997;18:35.
- Eckardt J, Gralla R, Palmer MC, et al. Topotecan as second-line therapy in patients with small cell lung cancer: a phase II study. Ann Oncol 1996;7:107.
- Eckardt J, Depierre A, Ardizzoni A, et al. Pooled analysis of topotecan (T) in the second-line treatment of patients (pts) with sensitive small cell lung cancer (SCLC). Proc Am Soc Clin Oncol 1997;16:452a.
- von Pawel J, Schiller JH, Shepherd FA, et al. Topotecan versus cyclophosphamide, doxorubicin, and vincristine for the treatment of recurrent small-cell lung cancer. J Clin Oncol 1999;17:658-67.
- Yamaoka T, Hanada M, Ichii S, et al. Cytotoxicity of amrubicin, a novel 9-aminoanthracycline, and its active metabolite amrubicinol on human tumor cells. Jpn J Cancer Res 1998;89:1067-73.
- Morisada S, Yanagi Y, Noguchi T, et al. Antitumor activities of a novel 9-aminoanthracycline (SM-5887) against mouse experimental tumors and human tumor xenografts. Jpn J Cancer Res 1989;80:69-76.
- Noguchi T, Ichii S, Morisada S, et al. Tumor-selective distribution of an active metabolite of the 9-aminoanthracycline amrubicin. Jpn J Cancer Res 1998;89:1061-6.
- Suzuki T, Minamide S, Iwasaki T, et al. Cardiotoxicity of a new anthracycline derivative (SM-5887) following intravenous administration to rabbits: comparative study with doxorubicin. Invest New Drugs 1997;15:219-25.
- Doxorubicin Hydrochloride for Injection. Kalamazoo, MI: Pharmacia & Upjohn Company, 2003.
- ELLENCE(R) intravenous solution, epirubicin intravenous solution. Kalamazoo, MI: Pharmacia & Upjohn Company, 2005.
- Makino Y, Yamamoto N, Sato H, et al. Pharmacokinetic and pharmacodynamic study on amrubicin and amrubicinol in Japanese patients with lung cancer. Cancer Chemother Pharmacol 2012;69:861-9.
- Available online: http://www.thomsonhc.com/micromedex2/librarian/PFDefaultActionId/evidencexpert.ShowDrugCompareResults
- Inoue K, Ogawa M, Horikoshi N, et al. Phase I and pharmacokinetic study of SM-5887, a new anthracycline derivative. Invest New Drugs 1989;7:213-8.
- Okamoto I, Hamada A, Matsunaga Y, et al. Phase I and pharmacokinetic study of amrubicin, a synthetic 9-aminoanthracycline, in patients with refractory or relapsed lung cancer. Cancer Chemother Pharmacol 2006;57:282-8.
- Onoda S, Masuda N, Seto T, et al. Phase II trial of amrubicin for treatment of refractory or relapsed small-cell lung cancer: Thoracic Oncology Research Group Study 0301. J Clin Oncol 2006;24:5448-53.
- Jotte R, Conkling P, Reynolds C, et al. Randomized phase II trial of single-agent amrubicin or topotecan as second-line treatment in patients with small-cell lung cancer sensitive to first-line platinum-based chemotherapy. J Clin Oncol 2011;29:287-93.
- Inoue A, Sugawara S, Yamazaki K, et al. Randomized phase II trial comparing amrubicin with topotecan in patients with previously treated small-cell lung cancer: North Japan Lung Cancer Study Group Trial 0402. J Clin Oncol 2008;26:5401-6.
- Nogami N, Hotta K, Kuyama S, et al. A phase II study of amrubicin and topotecan combination therapy in patients with relapsed or extensive-disease small-cell lung cancer: Okayama Lung Cancer Study Group Trial 0401. Lung Cancer 2011;74:80-4.
- Available online: www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/orphans/2009/11/human_orphan_000386.jsp&mid=WC0b01ac058001d12b

